







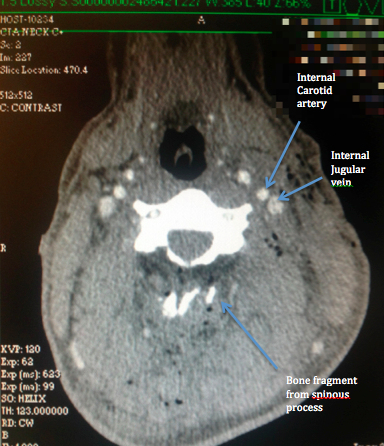
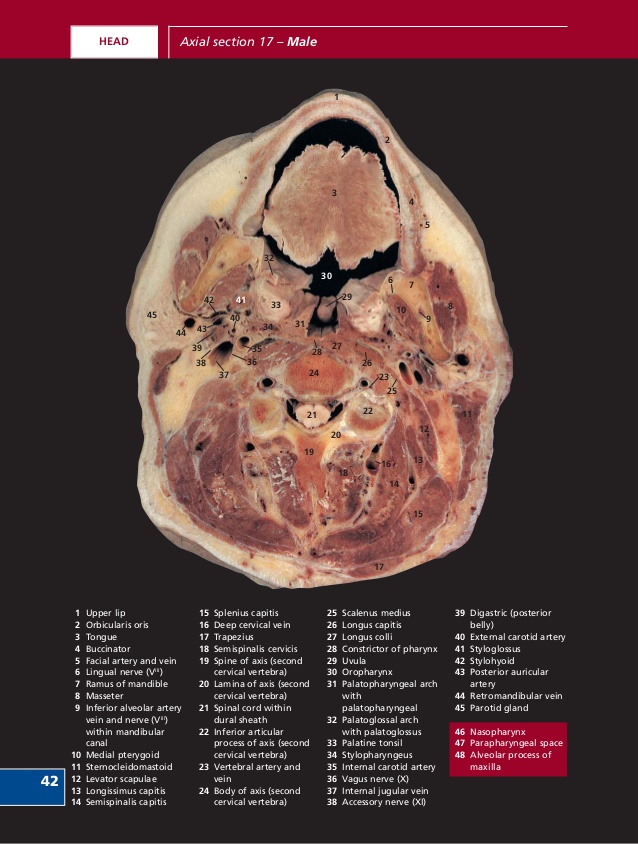
These next images show the path of the bullet through the neck, and the vital structures that the bullet somehow didn’t disrupt. Also included is an anatomy slide taken from the Internet, showing the gross structures at roughly the same level for comparison. In the first image, the path of the bullet can be seen by the small pockets of air drawn into the tissues as the bullet passed through, which appear black on the CT image. A blue line has been drawn along the bullet’s rough path to illustrate. The next image was taken after a dye was injected in the casualty’s veins, which pumped around his blood vessels, causing them to appear white on the CT scan.
Mentally superimposing the path of the bullet, it can be seen that it passes directly through a rather large pipe in the front of the casualty’s neck, which I assess as being the internal jugular vein. (I’m very happy to be corrected by any radiologists out there!) Immediately next to the internal jugular vein is an even more important structure, the internal carotid artery, which, had it been disrupted, would have almost certainly resulted in the death of the casualty given the circumstances on the day. Miraculously, neither of these major blood vessels were damaged, with the only rational explanation offered by the treating surgeon being that the bullet simply pushed them aside. Once again, in my opinion, were this to have been a M4 round, I suspect the outcome would have been dramatically worse.
So far I have only considered the damage done by the permanent cavity caused by the bullet, which both fractured the spinous process of the casualty’s vertebra and punched through the exact location of his major neck blood vessels without disrupting them. Of more medical significance, both on the day and ongoing since, was the damage done by the temporary cavitation of the bullet as it passed through. Those who have read my previous post (or have a good grasp of the subject) can disregard the following video, but for those who haven’t, the following YouTube video by Brass Fetcher demonstrates the pressure wave generated by a 7.62x39mm bullet when it passes through tissue. In the video, a bullet is shot into ballistic gelatin that has roughly the same density as human tissue. The pressure wave seen disrupting the gelatin in the video is caused as the bullet rapidly decelerates and transmits energy into the gelatin. The same occurs in human tissue with the pressure wave, or temporary cavity, causing damage to structures around, but not in the direct path of, the bullet.
The pressure wave emanating out from the path of the bullet through the casualty’s neck passed directly through his spinal cord. As it did so, the casualty went into a state of spinal shock, causing him to immediately lose all function of his nervous system below the injury and, while remaining conscious throughout the ordeal, making him temporarily quadriplegic. Spinal shock is often loosely referred to as a spinal concussion, similar to the temporary symptoms experienced following a knock to the head that gradually settle over a period of time. Thankfully, this was the case with the casualty in this case study, with the majority of his nervous system function returning in the hours post-injury, and a gradual recovery of almost all of his nervous functions after years of intensive rehabilitation.
Although making a steady recovery from the spinal shock in the months to years following the injury, a more insidious sequelae from the damage done by the temporary cavity of the bullet began to manifest. Interestingly from a medical perspective, the casualty developed symptoms of traumatic brain injury (TBI) which, while frequently seen in war casualties, is more typically associated with blast injuries, and almost always associated with loss of consciousness. Having spent my previous career in the military medical space, I had never heard of the concept of a TBI from a gunshot wound distal to the head. Having been introduced to the concept, however, and keeping the video image of the temporary cavitation from a high-velocity missile in mind, it makes perfect sense that that same pressure wave that disrupts tissues surrounding the permanent cavity of a bullet could cause significant damage to brain tissue, especially if shot at relatively close range through the neck or upper torso.
In fact, studies have demonstrated that ballistic wounds as distal as the abdomen and thorax can cause a transmitted pressure wave through the brain with enough force to generate a TBI (Courtney & Courtney, 2007). I encourage anyone reading this who has an interest in military medicine or TBIs to look up the Courtney reference, as it has opened my eyes to a new significant risk of TBI resulting from distal gunshot wounds that I was previously oblivious to, which has implications for early management of such injuries. With today’s heightened terrorist threat and recent world events, these military-related wounds may be presenting at a civilian emergency department near any one of us in the near future.
As stated in the introduction, fortunately this story has a happy ending in that the operator who was shot has gone from strength to strength in his recovery and is not showing any sign of slowing down. Frustratingly, despite being on the ground on the day of his injury, I was unable to get to him due to his geographical location and the tactical situation. The heroes of the day (apart from the casualty) were the first responders and the U.S. Aeromedical Evacuation team, who came into a highly complex and dangerous situation to extract the casualty under fire. TacMed Australia extends its sincere gratitude to all the pre-hospital medical practitioners and evacuation elements out there who save lives daily in civilian and military context alike.
As always, comments and questions are welcome.
![]()
References:
Apfelbaum JD, CS, Waldman N 2000, ‘Unstable cervical spine without spinal cord injury in penetrating neck trauma’, American Journal of Emergency Medicine, vol. 18, no. 1, pp. 55-57.
Courtney A, CM 2007, ‘Links between traumatic brain injury and ballistic pressure waves originating in the thoracic cavity and extremities’, Brain Injury, vol. 21, no. 7, pp. 657-662.
Lustenberger T, TP, lam L, Kobayashi L, Inaba K, Plurad D, Branco BC, Demetriades D 2011, ‘Unstable cervical spine fracture after penetrating neck injury: a rare entity in an analysis of 1,069 patients’, Journal of Trauma, vol. 70, no. 4, pp. 870-872.



COMMENTS