This case study details the experience of a DEA FAST agent who sustained a gunshot wound during a counter-narcotics operation in Southern Afghanistan. Despite the severity of the injury, he was able to return to duty within 36 hours after receiving prompt medical attention and following tactical casualty care principles.
Key points from this article:
The DEA FAST agent was shot by an AK47 round while engaged in a counter-narcotics operation targeting a Taliban-held village in Southern Afghanistan.
How the agent's quick decision to turn before boarding the helicopter likely saved his life by preventing a more severe injury to his head.
Why the principles of tactical casualty care are crucial, as demonstrated by the agent's rapid assessment and treatment, allowing him to return to duty just 36 hours after being shot.
Updating summary...
WATCH: DEA FAST agent shot during helicopter extraction under fire from Taliban drug raid
Dan Pronk
Speed
1x
Listen
COMMENTS
He turned up to work for the very next job, less than 36 hours after being shot!
This case study is of a good friend of mine (written with his consent) who sustained a through-and-through gunshot wound from an AK47 round from a range of approximately 200m. The operator who was shot was a DEA FAST agent, and my element and his were on a combined counter-narcotic job in Southern Afghanistan at the time. To set the scene, we had two targets to hit that day, the first of which was a raw opium deal in a Taliban-held village, and the second being the clearance of a known Taliban weapons and drugs cache.
Advertisement
We had planned a daytime raid for the first job as to catch the opium trade at the time that intelligence suggested it was taking place. The intel was good, and we were met with minimal resistance as we inserted on target, with the following photos showing some the haul of wet opium and IED components, including a bunch of low metal signature anti-personnel mines.
Advertisement
The Taliban had fled the center of town as we inserted, however as time passed on target they began to regroup in several compounds on the outskirts of town and started to engage us with harassing fire. As extraction approached the fire intensified and by the time the last helicopter of our extraction package landed we were engaged in a decent gunfight. Unfortunately the final extraction bird overflew the designated, and relatively protected, landing zone and landed in an exposed area approximately 200m from a cemetery in which several Talibs had taken up firing positions. The following video is of our chalk running to meet the extraction helicopter as it sits exposed in open ground. The operator who sustains the gunshot wound is the one who I kneel immediately next to. As luck would have it he chose the split second before he was shot to stand and turn to board the helicopter, causing the bullet to rip through his buttock and exit the front of his thigh, whereas it would have likely struck his head if he had remained kneeling.
As with any casualty in a tactical or high-threat environment the highest priorities are to control the threat situation if possible, minimize the likelihood of sustaining further casualties, or becoming a casualty yourself, and only then move on to casualty assessment and treatment. The video below demonstrates these principles in what has been coined by the Committee on Tactical Combat Casualty Care (CoTCCC) as Care Under Fire. The video is of a Reality Based Training (RBT) scenario in which an operator in the open has sustained a gunshot wound to the leg and is bleeding arterially. The responding operators assess the situation without exposing themselves to the fire-lane in which the simulated casualty has been shot. After encouraging the casualty to apply his own tourniquet and crawl to them, the responding operators use a combination of suppressing fire and smoke to suppress the threat and conceal the extraction of the casualty to a position of cover. From there a rapid assessment and treatment of only the immediately life-threatening injury is performed before further extracting the casualty to a safer locality.
Applying these principles to the original video, the highest priority after the casualty had been sustained was to continue to suppress the threat, load the casualty onto the helicopter, and then assess the casualty once we had launched back into the relative safety of the air.
Advertisement
In our pre-mission planning for the mission we had considered the possibility of sustaining casualties during all mission phases, including on extraction from the first target. As the flight time between Target 1 and Target 2 was approximately 10 minutes, the plan for that contingency was to do a rapid assessment of the casualty to determine if they were in need of immediate surgical intervention or not. This would then dictate whether we would divert our aircraft directly to a surgical facility or proceed to Target 2 and leave the casualty on board the helicopter to return for medical care once the remainder of us had inserted on the second target.
From the time I boarded the helicopter on extraction from Target 1 the clock was ticking to make that assessment. Despite the sub-optimal conditions in the back of the helicopter for casualty assessment, it was immediately evident that he was conscious, alert and talking, suggesting that his airway and breathing were not in immediate danger. The quick scrub done by other operators prior to me boarding the aircraft had identified a bleed in the casualty’s left buttock region, which was exposed by cutting away the casualty’s pants with trauma shears. Once exposed it was clear that the wound was not bleeding arterially, and was in no need of packing with any form of hemostatic dressing. Whilst I could see what appeared to be both an entrance and exit wound, my final concern was that the bullet may have fragmented and some might have entered his abdomen, as seen in the case study linked here. I have edited the video of the extraction prior to my full assessment of the casualty as not to show faces of fellow operators, but following what is seen on the video I conducted a brief assessment of the casualty’s abdomen to ascertain that there were no immediate signs of catastrophic internal bleeding. Once done, I relayed the message through to our headquarters element that the casualty was “Category Bravo” and didn’t need any immediate life-saving interventions. We proceeded to insertion on Target 2 and left the casualty on board the helicopter to return to base and get surgical attention.
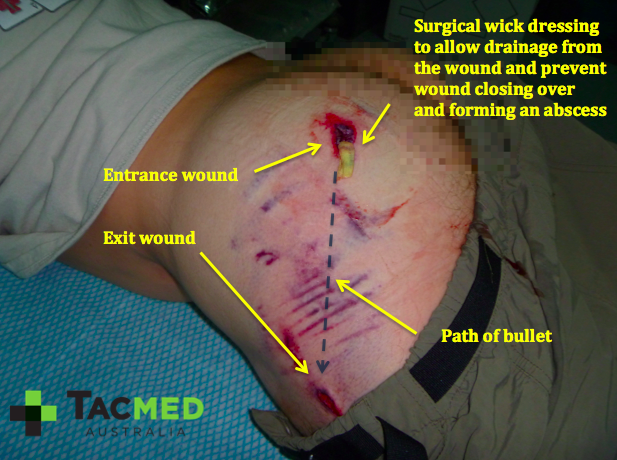
The casualty had an initial surgical clean-out of the wound when he returned to base and the tract of the bullet was packed with a wick dressing to allow it to continue to drain any infection out, rather that have it trapped in the tissues of the buttock to form an abscess. He turned up to work for the very next job, less than 36 hours after being shot!
36 hours following being shot, the casualty is back on an insertion bird seated to my left. To my right is fellow SOFREP author Mitch McAlister
The following images were taken at the end of that day. The early bruising from the temporary cavitation of the projectile dissipating energy into the tissues can be seen in these images, but is better appreciated in the next series of photos a few days later.
The series of photos below were taken at day 4 post-injury. Here it can be seen the extent of tissue damage radiating out from the path of the bullet as the temporary cavity pulverised small blood vessels it its path. For a detailed review of how high-velocity projectiles cause damage through permanent and temporary cavitation please see my previous article “Why I’d rather be shot by an AK47 than and M4.”
Photo credit: prism science.com
The photo above is a snapshot of a high-velocity projectile as it passes through ballistic gelatin calibrated to the density of human tissue. The pressure wave emanating out from the projectile causing the temporary distortion to the gelatin is what destroys small blood vessels immediately adjacent to the bullet tract and accounts for the bruising seen in the images below.
Despite antibiotics and daily wound cleaning and dressing changes, by day 7 post-injury the casualty’s wound had become infected. It can be appreciated that as the projectile passes through the human tissue it takes with it contaminants from the bullet itself, as well as the clothing that it has struck before entering the tissues, which in Afghanistan was always contaminated with dust with high fecal content. This coupled with the huge alternating positive and negative pressures associated with the temporary cavitation process seed these contaminants throughout the wound. The fact that the casualty (to his credit) continued to go out on jobs almost every day during the week following his wounding also made him a sitting duck for serious infection in the wound.
At day 7 we needed to give the wound a good scrub out and hit the casualty with a solid dose of intravenous antibiotics to get back on top of the infection. For anyone who has ever cleaned the barrel of a dirty rifle, the process of cleaning the casualty’s wound was remarkably similar. After a light anesthetic, a medical grade “bore cleaner” was used to scrub the wound out again and over the course of the next week the infection settled nicely allowing the wound to heal.
The principles discussed in this article about the immediate management of a casualty in a high-threat environment relate to a military context, however are as applicable to the civilian context. A good example of this is a car crash on a busy road. Applying the same principles, it is important to minimize the likelihood of further casualties, or becoming a casualty yourself by taking a few seconds to assess the scene before you respond. If there’s someone available to send up the road to warn traffic then that’s a great idea. Next step is to get on the phone and alert the authorities to get some help on the way. From there, assess as to whether there’s any immediate danger from the crashed car. Is it leaking fuel, or at risk of catching on fire? If so, this needs to be taken into consideration before engaging. Ideally after a car crash where spinal injuries are suspected the casualty should be stabilized in place and only moved once appropriate spinal precautions are in place. That said, if the casualty is in a car that is starting to catch fire, staying safe yourself and getting the casualty out to a place of safety are the highest priorities. Furthermore, as with our pre-mission planning in the case study above to prepare for the contingency of a casualty on extraction from Target 1, a bit of pre-mission planning for a car crash is not a bad idea. A small medical kit with an arterial tourniquet and a few pressure dressings tucked away in the trunk of your car will give you the very best chance of saving a preventable death in the instance that you’re on scene at a car crash before the paramedics. The same principles can be applied to hunting and camping trips; four-wheel driving in remote areas, a rock-climbing trip, and the list goes on…
As a sad aside, on Target 2 on the day of the case study we were once again met with fierce resistance and devastatingly lost one of our brothers. May he rest in peace and may we never forget the fallen.
Rest In Peace brother
As always, questions and comments are welcome.
Kind regards,
Dan
Advertisement
What readers are saying
Generating a quick summary of the conversation...
This summary is AI-generated. AI can make mistakes and this summary is not a replacement for reading the comments.
















COMMENTS